
Originally published in our book “Unready: To err is human – the other neglected side of Hospital Safety and Security” July, 2010 and as relevant four years later as it was on day one.
Due to length, we have broken this into two posts, of which this is the second. For context, it should be noted that this was written during the painful birth of the Department of Homeland Security. In retrospect, combining Public Health and the Non-Federal Healthcare Sector deserves questioning, especially as relates to All Hazards Security posture.
Myth: The Non-Federal Healthcare Sector has followed the Federal Healthcare Sector in All-Hazards Design and Construction of its Facilities.
Reality: As federal and metropolitan governments build more robust structures and mitigate safety and security vulnerabilities in their building environments, non-federal structures become more susceptible to terrorist attacks. Experts tell us that approximately 25% of all target selection is opportunity.
There is little need to discuss the role of design and construction in the sustainability of buildings in earthquake zones. The visual documentation of this year’s earthquakes in Haiti, Chile and Turkey and their devastating aftermath leaves little chance to trump with the printed word.
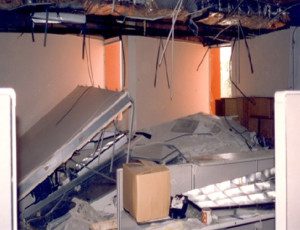 These events clearly demonstrate the unbelievable chaos that accompanies earthquake disasters. They also illustrate the need for advanced preparedness and the indispensable need for a unified command structure; if everyone is in control, no one is in control.
These events clearly demonstrate the unbelievable chaos that accompanies earthquake disasters. They also illustrate the need for advanced preparedness and the indispensable need for a unified command structure; if everyone is in control, no one is in control.
Great numbers of people ready to volunteer and huge piles of medical supplies and other items are necessary, but not sufficient, to respond to the immediate needs of suffering masses.
Earthquake zones in the U.S. have been identified. However, the U.S. Geological Survey experts, through no fault of their own, keep finding new earthquake fault connections. The All-Hazards Preparedness and Response community is most concerned about earthquake zones located in densely populated areas like the American West Coast – California, Oregon, Washington, Alaska, Hawaii – and in the Middle West New Madrid Fault Line areas – Missouri, Tennessee, Illinois, Kentucky, Mississippi, Georgia, and South Carolina.
The coastal areas are also subject to the dual hazards of earthquakes plus tsunamis. The destructive power of tsunamis has been visually documented through recent events in Indonesia, Malaysia, and Burma, with its death toll of over 230,000 individuals.
We cannot generalize hospital earthquake readiness based on concerns which have plagued this hospital industry in California. However, these concerns have surfaced repeatedly by those at risk in hospitals where structures have not been seismically upgraded.
Responding to the 1994 Northridge earthquake and the resulting damage to the area’s hospitals, the State legislative body mandated a robust program to seismically upgrade the State’s hospitals. It has been difficult to follow the political machinations by legislative actions. However, drop-dead dates for implementation of these seismic upgrades have had mixed results and leave many at risk.
A recent article in the Sacramento Bee leaves one with the impression that the “dust has not settled on the issue,†as evidenced in the caption, “California hospitals seek relief from seismic safety rules.†The California Hospital Association has petitioned to throw out the 2013 upgrade mandates.
 The California Nurses Association (CNA) is and has been a strong voice for action. They indicate that one-half of the existing hospitals need to be seismically upgraded. Other studies indicate that 47% of hospital floor space needing upgrades are in the Los Angeles and San Francisco Bay areas. We see little value in sharing the projected numbers of deaths and serious injuries, should the earth adjust its plates in this region. As a non-lawyer, we will not speculate on the level of risk exposure this scenario represents.
The California Nurses Association (CNA) is and has been a strong voice for action. They indicate that one-half of the existing hospitals need to be seismically upgraded. Other studies indicate that 47% of hospital floor space needing upgrades are in the Los Angeles and San Francisco Bay areas. We see little value in sharing the projected numbers of deaths and serious injuries, should the earth adjust its plates in this region. As a non-lawyer, we will not speculate on the level of risk exposure this scenario represents.
Since disparate groups are at loggerheads about how society deals with the many arcane legal, ethical, and moral judgments in protection of a trusting public, it seems necessary that these disparities must be put aside in the face of these obvious dangers. Long-time observers say that the current argument that funds are not available in “lean times†rings hollow, seeing that they were not made available during earlier fat times.
The existence of what the nurses call an Occupational Safety and Health Act (OSHA) violation in “known unsafe workplaces†does not appear to impact on DHHS (conditions of participation) or “deemed status†eligibility to receive payment for the care of federal beneficiaries. The same may be said for selection as one of the “best of breed†from the growing cottage industry of a hundred best of “this and that.†Organizations that presume to guide a trusting public to the best quality and safety for healthcare should take great care to factor in physical safety of that locus of care.




0 Comments